Figures
Abstract
Background
Clinical observations and animal studies have suggested that Salmonella intestinal carriage is promoted by concurrent Schistosoma infection. The present study assessed association of Salmonella intestinal carriage and Schistosoma mansoni infection among individuals in a Schistosoma endemic area in sub-Saharan Africa.
Methods
From November 2015 to March 2016, a cross-sectional community-wide study was conducted in Kifua II, a rural village in Kongo Central Province, Democratic Republic of Congo. Stool samples were collected and analyzed for Salmonella intestinal carriage (culture) and Schistosoma mansoni infection (Kato Katz microscopy with determination of egg load). Salmonella Typhimurium and Enteritidis isolates were assessed for genetic similarity with blood culture isolates obtained during the same period in a neighboring hospital using multi-locus variable-numbers tandem repeat analysis (MLVA).
Results
A total of 1,108 participants were included (median age 15 years (IQR: 7–36), male-to-female ratio of 1:1.1). The overall prevalence of Schistosoma mansoni infection and non-typhoidal Salmonella carriage was 51.2% (95% CI: 48.2–54.1) and 3.4% (95% CI: 2.5–4.7) respectively, with 2.2% (95% CI: 1.5–3.2) of participants coinfected. The proportion of Salmonella carriage tended to be higher among Schistosoma mansoni infected participants compared to non-infected participants but this difference did not reach statistical significance (4.2% versus 2.6%, p = 0.132). However, the proportion of Salmonella carriage among participants with a heavy Schistosoma mansoni infection was significantly higher compared to those with a light and moderate infection (8.7% versus 3.2%, p = 0.012) and compared to Schistosoma mansoni negatives (8.7% versus 2.6%, p = 0.002). The 38 Salmonella isolates comprised five and four Enteritidis and Typhimurium serotypes respectively, the majority of them had MLVA types identical or similar to those observed among blood culture isolates.
Author summary
Salmonella intestinal carriage may be facilitated by infection with Schistosoma mansoni, which is a flatworm that lives in the small blood vessels of the human intestinal tract. This situation has been described in tropical low and middle income countries, where both pathogens are endemic. The present study aimed to assess the association of Salmonella intestinal carriage with Schistosoma mansoni infection in Kifua II village, located in the Kongo Central province of the Democratic republic of Congo. We collected stool samples from 1,108 inhabitants of the village and analysed them for Salmonella (culture) and Schistosoma mansoni eggs (microscopy). Our findings showed that 3.4% of the participants had Salmonella in their stool and 51.2% were infected with Schistosoma mansoni. There was no association between overall Schistosoma infection and Salmonella carriage but Salmonella carriage was significantly higher among participants with heavy Schistosoma infection compared to those with a light and moderate infection (8.7% versus 3.2%, p = 0.012) and compared to those without Schistosoma mansoni infection (8.7% versus 2.6%, p = 0.002). Further, we showed that some Salmonella isolates recovered from stool were very similar to isolates obtained from invasive infections (blood cultures from patients in a neighbouring hospital).
Citation: Mbuyi-Kalonji L, Barbé B, Nkoji G, Madinga J, Roucher C, Linsuke S, et al. (2020) Non-typhoidal Salmonella intestinal carriage in a Schistosoma mansoni endemic community in a rural area of the Democratic Republic of Congo. PLoS Negl Trop Dis 14(2): e0007875. https://doi.org/10.1371/journal.pntd.0007875
Editor: James B. Lok, University of Pennsylvania, UNITED STATES
Received: May 30, 2019; Accepted: October 25, 2019; Published: February 21, 2020
Copyright: © 2020 Mbuyi-Kalonji et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: All data are available on Figshare, using the link: https://figshare.com/articles/Nontyphoidal_Salmonella_intestinal_carriage_in_a_Schistosoma_mansoni_endemic_community_in_a_rural_area_of_the_Democratic_Republic_of_Congo/11695152
Funding: This work was funded by the Belgian Directorate of Development Cooperation (DGD) through the 3rd and 4th Framework Agreement between the Institute of Tropical Medicine in Belgium, Antwerp, Belgium and the National Institute for Biomedical Research, Kinshasa, Democratic Republic of the Congo as well as by the Baillet-Latour Fund. LK holds a PhD scholarship from the Belgian DGD and ASH holds a PhD scholarship from the Research Foundation Flanders. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests: The authors have declared that no competing interests exist.
Introduction
In sub-Saharan Africa, Salmonella is among the most frequent bacteria causing invasive infections in humans [1,2]. Invasive Salmonella infections comprise the human-restricted typhoid fever (caused by Salmonella enterica subspecies enterica serotypes Typhi and Paratyphi) as well as the non-typhoidal Salmonella (NTS) infections. Invasive NTS mainly include two serotypes: Salmonella enterica serotype Typhimurium (Salmonella Typhimurium) and Salmonella enterica serotype Enteritidis (Salmonella Enteritidis). In 2010, 11.9 million typhoid fever cases were reported worldwide causing 129,000 deaths [3,4]. Typhoid fever incidence in sub-Saharan Africa is more than 100 cases per 100,000 person-years [3,4]. The global burden of non-typhoidal Salmonella is even higher, with 3.4 million cases reported worldwide in 2010, mainly affecting children < 5 years old and resulting in an estimated 680,000 deaths [5].
The pivotal role of human carriers in the transmission of typhoid fever is well-known [1,6,7]. In contrast, Salmonella Typhimurium and Salmonella Enteritidis infect a broad range of vertebrate animals and the reservoir of both serotypes is considered to be zoonotic [1]. However, there is evidence that both serotypes have genetically adapted to the human host [8], putting forward the possibility of a human reservoir. With regard to Salmonella intestinal carriage, it is defined as excretion of Salmonella in stool in absence of symptoms of infection; and those individuals who excrete the bacteria in their stool are called “Salmonella carriers” [9]. This situation has been described in typhoidal as well as non-typhoidal serovars. In contrast to typhoid fever, little is known about the frequency and duration of non-typhoidal Salmonella carriage after infection in sub-Saharan Africa [2].
Schistosomiasis is a neglected tropical disease caused by parasitic worms with freshwater snails as intermediate hosts. Schistosoma mansoni is one of the main species infecting humans; its adult worms live in the mesenteric capillaries [10]. Without treatment, Schistosoma mansoni infection may result in hepatosplenic inflammation and liver fibrosis [11].
There is clinical and experimental evidence towards a symbiotic relation between Schistosoma and Salmonella and associations have been described for different Schistosoma species and both Typhi and NTS serotypes. Clinical observations in patients from Egypt and Gabon showed that, in the presence of Schistosoma infection, relapsing or persistent Salmonella bacteremia or bacteriuria were only cured when concomitant anti-Schistosoma treatment was given [12–14]. Furthermore, hospital case series and cross-sectional studies from Nigeria and Egypt showed an overrepresentation of Schistosoma infections among patients with invasive salmonellosis [10,13] as well as an overrepresentation of Salmonella infection among Schistosoma-infected patients [15]. However, these studies had limitations. For example, patient groups were ill-defined and control groups were absent [10,12,13,15,16]. In addition, different reference tests were used including the Widal test which is based on typhoidal Salmonella (Typhi and Paratyphi) antibody detection and is not recommended as a diagnostic test in endemic settings [10,15]. Lastly, patients were given antibiotic treatments such as amoxicillin or chloramphenicol which are ineffective to prevent relapses [12,14,16]. These limitations preclude inter-study comparison and sound conclusions. Of note, a study in Malawi conducted in a cohort of HIV-infected patients, failed to demonstrate a clinical association between Salmonella and Schistosoma infections in terms of Salmonella recurrence and mortality [17].
Experimental studies demonstrated that Salmonella bacteria (mainly Paratyphi A and Typhimurium) were able to colonize adult Schistosoma worm by connecting their fimbrial protein (FimH) to a receptor located on the worm teguments [18–22]. Furthermore, increased morbidity and mortality were observed in co-infected mice and hamsters [18,20,23–27]. In addition, the physical association of Salmonella with Schistosoma worms was shown to increase the inhibitory concentrations of several classes of antibiotics [22]. Finally, alteration of the macrophage function in S. mansoni-infected mice was observed and this was related to growth and survival of Salmonella Typhimurium [28]. However, many of these experimental studies used very high doses of Salmonella injected intravenously, intraperitoneally or intracardially [18,21,24].
Despite the fact that well-designed epidemiological studies on Salmonella-Schistosoma coinfections are lacking, there is concern that concurrent Schistosoma infection may interfere with effectiveness of typhoid vaccines [29] and by extension with the future non-Typhoidal Salmonella vaccines.
In the Democratic Republic of Congo (DRC), located in Central-Africa, schistosomiasis and invasive Salmonella infections are endemic [30–35]. The main objective of the present study was to assess the prevalence of Salmonella intestinal carriage in a Schistosoma mansoni endemic community, and to assess a possible association between both pathogens. Additional objectives were to assess the serotype distribution of the intestinal Salmonella isolates and their genetic relatedness with invasive (blood culture) isolates.
Methods
Ethics statement
The study protocol was approved by the Institutional Review Board at the Institute of Tropical Medicine in Antwerp (Reference 852/12), the ethical committee of University of Antwerp (Reference 12/50/423) and the ethical committee of the Public Health School of Kinshasa, in the Democratic Republic of the Congo (References ESP/CE/022B/14 and ESP/CE/022C/2015). The study team obtained authorizations from the DRC ministry of health and the local authorities of the Kongo Central province. Before starting, the aim of the study and its benefits were explained to the community. All eligible adult participants were asked for written informed consent; children between 15 and 18 years old of age were additionally asked for written assent. For children under 15 years old, written informed consent from the legal representative was obtained.
Study site
The province of Kongo Central in DRC reported invasive Salmonella infections decades ago [36] but also more recently [33,37]. The area is also endemic for schistosomiasis with a predominance of Schistosoma mansoni infection [35]. After the assessment of six Health Reference Zones in the Province of Kongo Central during site visits, the village of Kifua II (-5°25´42.1”S; 14°39´19.1”E) situated in the health area of Tumba Misson and in the Health Zone of Kwilu Ngongo was selected as the study site (Fig 1). The study area extended over a surface of 196,560.90 m2 and had a population of about 1,400 inhabitants. The specific prevalence of HIV in the study population was not known however, in DRC the endemicity of HIV is less than 1% [38]. Prior to our study, no mass drug administration for the control of schistosomiasis had taken place. Kifua II is easily accessible by car, allowing for timely transport of stool samples to the laboratory of the reference hospital of Kimpese (Institut Médico-Evangélique of Kimpese, IME-Kimpese) at 35 km distance.
Kifua II village, health area of Tumba Mission, Health Zone of Kwilu Ngongo. https://www.caid.cd/graphics/province/12_Kongo-Central.png.
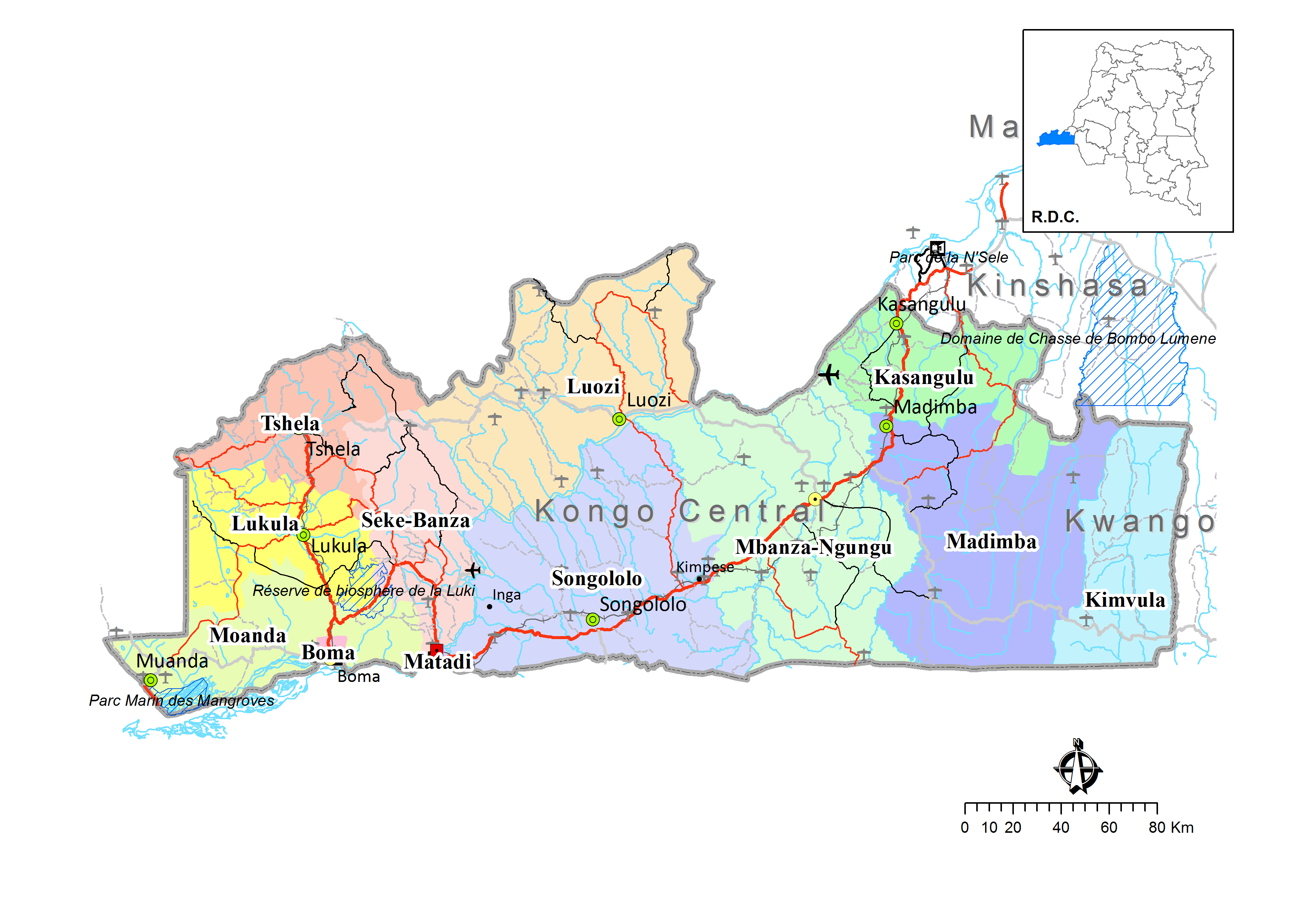{kind=link}
Study design
This study was conducted from November 2015 to March 2016, during the rainy season, which is expected to have the highest number of Salmonella infections. It was embedded in an eco-epidemiological cross-sectional study on helminth co-infections and related morbidity patterns in a rural area of DRC. All inhabitants living for more than 1 year in Kifua II village and being more than 1 year old were eligible and were invited to participate in the study. The study team went to the village early morning to reach participants before they departed for field work. After giving informed consent, each participant was asked to give two consecutive stool samples within 1 week. Participants (or their caretakers) were also interviewed about demographics and recent history of fever (≤ 14 days), diarrhea (24 hours before enrollment) and antibiotic treatment (≤ 48 hours before enrollment).
Detection of Schistosoma mansoni infection
Within 2 hours upon arrival at the laboratory of IME-Kimpese, stool samples were processed by the Kato Katz method (2 slides of 25 mg of fecal material for each stool sample, with a maximum of 4 slides per participant) and within 24 hours, slides were microscopically examined for the presence and number of Schistosoma mansoni eggs. The sum of the egg count from 4 slides was multiplied by 10 to reach one gram of stool. The Schistosoma mansoni infection intensity was expressed as the number of eggs detected per gram of feces (EPG). According to WHO guidelines, Schistosoma infection intensity was categorized as light, moderate or heavy at egg counts of 1–99 EPG, 100–399 EPG or ≥ 400 EPG, respectively [39].
One dose of 40mg/kg of praziquantel was administered to all inhabitants of the community at the end of the study.
Detection of Salmonella carriage
Within 2 hours after sample reception at Kifua II health center, approximately 1 gram of each stool sample was suspended into 10 ml of selenite broth (BD Difco, Becton Dickinson and Company, Franklin Lakes, New Jersey). After that, all samples were transported to the laboratory of IME-Kimpese. Upon arrival, the selenite broth tubes were incubated for 18 hours at 35°C, then, 10 μl was sub-cultured on each of two plates of Salmonella-Shigella agar (SS) (Lab M Limited, Lancashire, United Kingdom). After incubation (18–24 hours at 35°C), colonies suspected for Salmonella (lactose negative with H2S positive center) were sub-cultured on Kligler Iron Agar (KIA) (Lab M Limited) for 18–24 hours at 35°C. Per suspected colony type, two colonies were sub-cultured on KIA with a maximum of four colony types per SS agar plate. In case of no growth on the SS agar, the plates were read after another 24 hours of incubation. Bacterial isolates from KIA tubes showing a pattern suggestive of Salmonella (glucose fermentation, lactose negative, H2S positive) were inoculated in a gallery consisting of three disk-based biochemical tests (DiaTabs, Rosco, Taastrup, Denmark): ortho-nitrophenyl galactopyranoside (ONPG), urease and lysine decarboxylase (LDC) combined with indole production. Isolates with a reaction pattern compatible with Salmonella (ONPG negative, urease negative, LDC positive and indole negative) were stored on 2-ml tubes with Trypticase Soya Agar (TSA, OXOID, Basingstoke, United Kingdom) and shipped to the National Institute of Biomedical Research (INRB, Kinshasa, DRC) and the Institute of Tropical Medicine (ITM, Antwerp, Belgium) for confirmation, serotyping (VisionTM, Pro-lab Diagnostics Inc., Richmond Hill, Ontario, Canada) and antibiotic susceptibility testing (AST). AST was performed by disk diffusion (Neo-Sensitabs, Rosco) according to the Clinical and Laboratory Standards Institute (CLSI) M100-S27 criteria (40). For ciprofloxacin and azithromycin, minimal inhibitory concentration (MIC) values were determined using the E-test macromethod (bioMérieux, Marcy L’Etoile, France) with breakpoints according to the CLSI guideline [40]. Multidrug resistance (MDR) was defined as co-resistance to the three first-line antibiotics (ampicillin, chloramphenicol and trimethoprim-sulfamethoxazole) [41].
It was decided not to treat Salmonella Typhi intestinal carriers with antibiotics given the (i) high endemicity of typhoid fever in sub-Saharan Africa (with a consequently less important role of household intestinal carriers in transmission) [46] and the (ii) high doses/long period of required ciprofloxacin treatment combined with its safety profile [47]. Likewise, antibiotic treatment was not installed for NTS carriers, with the additional argument that stool shedding of NTS is mostly of short duration [48,49].
Salmonella multi-locus variable-numbers tandem repeat analysis (MLVA)
Salmonella Typhimurium (n = 4) and Salmonella Enteritidis isolates (n = 5) were sent to the Institute of Public health (IPH, Brussels, Belgium) for multi-locus variable-numbers tandem repeat analysis (MLVA) as previously described [42–44]. MLVA profiles were attributed based on the number of tandem repeats on five loci (SENTR7, SENTR5, SENTR6, SENTR4, SE3 for Salmonella Enteritidis and STTR9, STTR5, STTR6, STTR10, STTR3 for Salmonella Typhimurium isolates). In addition, Salmonella Typhimurium and Salmonella Enteritidis isolates (n = 19 and n = 10 respectively) recovered from a blood culture surveillance performed at the referral hospital of Kisantu (at 66 km from Kifua II) were used for comparison of MLVA types; isolates were representative for time (period September 2015 –December 2016) and antibiotic susceptibility profile. MLVA patterns were compared for genetic relatedness: a Typhimurium cluster was defined as isolates with variation in none or one of the rapidly changing loci (STTR5, STTR6 and STTR10) and no variation in the stable loci (STTR3 or STTR9) [45]; an Enteritidis cluster was defined as isolates with variation in none or one of the five loci [43]. A major MLVA type was defined as MLVA profiles comprising more than one Salmonella isolate.
Data collection and analysis
Field data and laboratory results were registered into case report forms and laboratory registers.
Data entry and analysis were done using Excel 2016 (Microsoft, Richmond, US). Duplicate Salmonella isolates from consecutive samples were removed from analysis. Data were characterized by frequencies, proportions, medians, interquartile range (IQR) and 95% confidence interval (95% CI). Chi-square test or Fisher exact test were used to test the association between Salmonella and Schistosoma mansoni infection. Results were considered significant when the p-value was < 0.05.
Results
Study population
In the village Kifua II, there were 1,304 eligible inhabitants among whom 196 (15%) did not participate to the study. Main reasons of non-participation were absence from the site (113/196) and refusal (55/196). Among 1,136 inhabitants who gave consent, 1,108 provided at least one stool sample. Their median (IQR) age was 15 (7–36) years, with a male-to-female rate of 1:1.1. Of them, 865 (78.0%) provided a second stool sample (S1 Fig). Of the participants answering the different questions of the survey, 3.2% (36/1,108) reported use of antibiotics within 48 hours before enrollment, 2.6% (29/1,108) and 21.3% (236/1,108) reported a history of diarrhea and fever within 14 days before enrollment, respectively. Salmonella carriage was neither associated with recent history of fever (8/38 versus 222/1,031, p = 0.943) nor with diarrhea (1/38 versus 28/1,030 p = 0.974) and none of the Salmonella carriers had taken antibiotics within 48 hours before enrollment.
Schistosoma mansoni infection
More than half of the participants (51.2%, 567/1,108; 95% CI: 48.2–54.1) were Schistosoma mansoni positive; infection intensities were light, moderate and heavy in respectively 51.3%, 30.5% and 18.2% (Table 1).
Salmonella intestinal carriers
A total of 38 participants were detected as Salmonella carriers, representing an overall carriage rate of 3.4% (95% CI: 2.5–4.7) of the study population. The number of Salmonella isolates among the first and second samples was 25/1,108 (2.3%) and 14/865 (1.6%) respectively. One patient (male, 56 years old) had a stool sample grown with Salmonella Kisarawe in both samples (second sample submitted 1 day after the first sample). Salmonella carriage was neither associated with recent history of fever (8/38 versus 222/1,031; p = 0.943) nor with diarrhea (1/38 versus 28/1,030; p = 0.974) and none of the Salmonella carriers had taken antibiotics within 48 hours before enrollment.
Salmonella intestinal carriage in relation to Schistosoma mansoni infection
Among the 38 Salmonella carriers, 24 participants were coinfected with Schistosoma mansoni, representing 2.2% (95% CI: 1.5–3.2) of the total study population. The proportion of Salmonella carriage among Schistosoma infected participants tended to be higher (4.2%, 24/567; 95% CI: 2.9–6.2) compared to Schistosoma non-infected participants (2.6%, 14/541; 95% CI: 1.6–4.3) but this difference did not reach statistical significance (p = 0.132). Moreover, the proportion of Salmonella carriers among Schistosoma-infected participants with heavy infection intensity (8.7%, 9/103; 95% CI: 4.7–15.8) was significantly higher than the proportion among those with light and moderate infection intensities combined (3.2%, 15/464; 95% CI: 1.9–5.3; p = 0.012). It was also higher than the proportion of Salmonella carriers among the Schistosoma negative participants (2.6%, 14/541; p = 0.002) (Table 1).
Serotype distribution of Salmonella isolates
Among the 38 Salmonella isolates (Table 2), 15 different serotypes were found of which Salmonella Stanleyville and Salmonella Enteritidis represented five isolates each. Salmonella Typhimurium and Rubislaw represented four isolates each. Salmonella Typhi was not found. There were two households in which two participants were carrier of the same serotype (Salmonella Typhimurium and Salmonella Kisarawe respectively), otherwise no particular clusters were seen. MDR was only observed among Salmonella Typhimurium and Salmonella Enteritidis (4/4 isolates and 1/5 isolates respectively). All isolates were susceptible to ciprofloxacin, tetracycline, ceftriaxone and azithromycin.
There was no association between Salmonella serotype and Schistosoma co-infection. Although the numbers were too small to trace associations, it was observed that three out of five MDR isolates occurred among children < 5 years old. Likewise, Salmonella Typhimurium tended to occur more among children < 15 years old (3/4 isolates), whereas non-MDR Salmonella Enteritidis occurred more frequently among adults (3/4 isolates).
MLVA typing of intestinal and blood culture Salmonella Typhimurium and Enteritidis isolates
The four Salmonella Typhimurium intestinal isolates were compared to 19 blood culture isolates. Six major MLVA types and four other MLVA types (comprising only one isolate) were observed. Three out of four intestinal Typhimurium isolates shared similar MLVA types with blood culture isolates (Fig 2). The five Salmonella Enteritidis intestinal isolates were compared to 10 blood culture isolates and yielded three major MLVA types. Two out of five intestinal Enteritidis isolates shared identical or similar MLVA types with blood culture isolates (Fig 3).
Position of the isolates along the timeline represents the time of isolation in 2015 or 2016. Series of 5 numbers represent 5 loci on which each number corresponds to the numbers of alleles amplified and “NA” corresponds to a locus on which no allele has been amplified. Symbol “†” denotes highly related MLVA types among intestinal and invasive isolates.
Position of the isolates represents the time of isolation in 2015 or 2016. Series of 5 numbers represent 5 loci on which each number corresponds to the numbers of alleles amplified and “NA” corresponds to a locus on which no allele has been amplified. Symbol “†” denotes highly related MLVA types among intestinal and invasive isolates. Symbol “*” denotes identical MLVA types among intestinal and blood culture isolates.
Discussion
The present study was conducted in a Schistosoma mansoni endemic community in a rural area in DRC. Results showed a prevalence of intestinal Salmonella-Schistosoma co-infections of 2.2% in the study population. The percentage of Salmonella intestinal carriage tended to be higher among Schistosoma-infected than among Schistosoma non-infected participants (4.2% versus 2.6%). Furthermore, the proportion of Salmonella carriage was significantly higher among participants with a heavy Schistosoma mansoni infection intensity (8.7%) compared to those with light and moderate infection intensities (3.2%). Among 38 Salmonella isolates (overall carriage rate of 3.4%), Enteritidis and Typhimurium serotypes were found (n = 5 and n = 4 respectively), most of which had MLVA types identical or similar to those from blood cultures.
The present findings add to the evidence of an association between Schistosoma mansoni infection and Salmonella intestinal carriage. The fact that the association between Schistosoma and Salmonella mainly occurred among the heavy infection intensity group fits with clinical observations of co-infections in long-standing or serious Schistosoma infections [14,50].
Previous community-based studies among asymptomatic participants reported a Schistosoma-Salmonella association in two cross-sectional surveys in Nigeria, reporting 4.4% and 5.4% of Schistosoma mansoni–Salmonella co-infected participants [13,51]. Two studies from Sudan reported 30.9% and 60.0% of Salmonella Typhi/Paratyphi excretion in urine or stool among Schistosoma-infected patients [52,53]. However, in both studies, control groups were not assessed for Salmonella carriage and in none of the aforementioned studies were selection and representativeness of the participants described.
In our study, the overall Salmonella carriage rate was 3.4%, and only non-typhoidal Salmonella were isolated. Few studies from sub-Saharan Africa have addressed Salmonella intestinal carriage, and most have addressed food handlers and related professions [54]. In recent community surveys in Guinea-Bissau and Senegal, Salmonella intestinal carriage rate was 2.4% and 1.0% respectively [54]. These lower proportions may be explained by the fact that in these surveys only a single stool sample per participant was assessed as well as by a difference in access to safe water supply and sanitation.
Most intestinal Salmonella isolates belonged to serotypes different from the invasive Typhimurium and Enteritidis serotypes [33]. However, both invasive serotypes (n = 9) accounted for a quarter of the intestinal isolates and represented 0.8% (9/1,108) of the overall study population. Most of them had MLVA types identical or similar to those of the blood culture isolates obtained in the same period from a hospital at 66 km distance. It may be expected that, if the blood culture surveillance had been conducted closer to Kifua II, even a better concordance of intestinal and invasive Typhimurium and Enteritidis MLVA types would have been observed. This observation adds to the evidence of the human nature (reservoir and potentially transmission) of the invasive Typhimurium and Enteritidis NTS serotypes.
The present study has some limitations. First, for logistical reasons only a maximum of two successive stool samples per patient were requested. In view of the intermittent excretion of Salmonella organisms, three successive stool samples would have been optimal [49,55] and could have yielded higher proportions of Salmonella carriage and Schistosoma mansoni infections. However, obtaining three successive samples in field studies may be challenging due to participant reluctance [55]. Of note, previous studies assessing Schistosoma-Salmonella interactions were mostly based on only one stool sample per participant [10,13,51]. Likewise, Schistosoma eggs excretion may have variations and the proportion of light Schistosoma infections could have been higher, as the Kato Katz method tends to be false-negative at low egg loads [55]. Immunological methods such as circulating cathodic antigen (CCA) detection in urine are promoted for the diagnosis of Schistosoma mansoni infection in endemic communities. The CCA-point-of-care test is related to the intensity of infection but does not express egg load [56,57]. In addition, it would not have provided better results than microscopy, as it may be false negative in light infections and requires more than one sample for optimal sensitivity [55].
A second limitation of this study is the small number amount of Salmonella carriers, which did not allow to reach statistical significance in the assessment of the overall association between Salmonella carriage and Schistosoma infection. The third limitation is that we did not assess possible associations between Salmonella and other species of Schistosoma such as Schistosoma haematobium [50].
A strength of the present study is that it is, to our knowledge, the first population-based study on the association of Salmonella intestinal carriage with Schistosoma mansoni infections in Central Africa. Moreover, sample work-up including sample transport conditions and delays were well controlled and complied with the prescribed norms [58]. Furthermore, unlike previous studies, the association between Schistosoma mansoni infection intensity and Salmonella carriage was investigated as well as the distribution of Salmonella serotypes and their genetic relatedness with invasive isolates.
The impact of this study for the control of invasive salmonellosis may be summarized as follows: even among heavy Schistosoma mansoni infections, the proportion of invasive Salmonella serotypes (Typhimurium and Enteritidis) was still low. Based on the present findings, Schistosoma mansoni infection is not expected to constitute a barrier to immunization of populations by Salmonella vaccination as mentioned in a recent review [29]. Further studies are needed to confirm the present findings for other Schistosoma species and Salmonella-infected patients (bacteremia and bacteriuria).
Acknowledgments
We would like to thank the persons who highly contributed to this study, especially the Medical Doctor Head of the Kwilu Ngongo Health Zone, for his participation to the mass sensitization of the Kifua II village inhabitants; we are grateful to the health committee of Kifua II village for their participation to the individual sensitization and collection of samples. We are sincerely thankful to Sylvain Baloji, from the Department of Epidemiology at the National Institute for Biomedical Research in Kinshasa, for his hard and dedicated work during field activities. We wish to thank the laboratory team of Institut Médico-Evangélique de Kimpese for their participation to the bacteriological and parasitological analysis.
References
- 1. Gal-Mor O, Boyle EC, Grassl GA. Same species, different diseases: How and why typhoidal and non-typhoidal Salmonella enterica serovars differ. Vol. 5, Frontiers in Microbiology. 2014.
- 2. Haeusler GM, Curtis N. Non-typhoidal salmonella in children: Microbiology, epidemiology and treatment. Adv Exp Med Biol. 2013;764.
- 3. Crump JA, Sjölund-Karlsson M, Gordon MA, Parry CM. Epidemiology, clinical presentation, laboratory diagnosis, antimicrobial resistance, and antimicrobial management of invasive Salmonella infections. Vol. 28, Clinical Microbiology Reviews. 2015.
- 4. Marks F, von Kalckreuth V, Aaby P, Adu-Sarkodie Y, El Tayeb MA, Ali M, et al. Incidence of invasive Salmonella disease in sub-Saharan Africa: a multicentre population-based surveillance study. Lancet Glob Heal. 2017;5(3).
- 5. Ao TT, Feasey NA, Gordon MA, Keddy KH, Angulo FJ, Crump JA. Global burden of invasive nontyphoidal Salmonella disease, 20101. Emerg Infect Dis. 2015;21(6).
- 6. Mogasale V, Ramani E, Mogasale V V., Park JY. What proportion of Salmonella Typhi cases are detected by blood culture? A systematic literature review. Annals of Clinical Microbiology and Antimicrobials. 2016.
- 7. Pui CF, Wong WC, Chai LC, Nillian E, Ghazali FM, Cheah YK, et al. Simultaneous detection of Salmonella spp., Salmonella Typhi and Salmonella Typhimurium in sliced fruits using multiplex PCR. Food Control. 2011;22(2).
- 8. Feasey NA, Dougan G, Kingsley RA, Heyderman RS, Gordon MA. Invasive non-typhoidal Salmonella disease: An emerging and neglected tropical disease in Africa. The Lancet. 2012.
- 9. Sirinavin S, Jayanetra P, Thakkinstian A. Clinical and Prognostic Categorization of Extraintestinal Nontyphoidal Salmonella Infections in Infants and Children. Clin Infect Dis. 1999;
- 10. Modebe AA, Nnachi AU, Ukaegbu CO, Tata N, Agah M V, Udu-Ibiam OE, et al. Dual infections of Enteric Salmonella species with Schistosoma mansoni among Patients from Two Hospitals in Jos, Nigeria. J Appl Environ Microbiol. 2014;2(4):198–202.
- 11. Gryseels B, Polman K, Clerinx J, Kestens L. Human Schistosomiasis. HHS Public Access. 2015;383(9936):2253–64.
- 12. Gendrel D, Richard-Lenoble D, Rombila M, Engohan E, Nardou M, Moussa You A, et al. Schistosoma intercalatum and Relapses of Salmonella Infection in Children. Am J Trop Med Hyg. 1984;33(6):1166–9. pmid:6439063
- 13. Igwe NN, Agbo EA. Incidence of co-infection of enteric Salmonella with Schistosoma in Kachia Local Government Area of Kaduna State, Nigeria. Int J Trop Med Public Heal. 2014;3(1):12–7.
- 14. Chacha F, Mshana SE, Mirambo MM, Mushi MF, Kabymera R, Gerwing L, et al. Salmonella Typhi meningitis in a 9-year old boy with urinary schistosomiasis: a case report. BMC Res Notes. 2015;8(1).
- 15. Nwaugo VO, Nduka FO, Nwachukwu NC. Concomitant typhoid infection in urinary schistosomiasis in South Estern Nigeria. Glob J pure Appl siences. 2005;11(3):353–6.
- 16. Gendrel D, Richard-Lenoble D, Rombila M, Engohan E, Nardou M, Moussa You A, et al. Non-typhoidal Salmonella septicemia in gabonese children infected with Schistosoma haematobium. Clin Infect Dis. 1994;18:103–5. pmid:8054417
- 17. Gordon MA, Visser L, Zijlstra EE, Molyneux M. Schistosomiasis Does Not Contribute to Death or Recurrence of Nontyphoid Salmonella Bacteremia in Human Immunodeficiency Virus–Infected Malawian Adults. Clin Infect Dis. 2003;37:e177–9. pmid:14689364
- 18. Collins FM, Boros DL, Warren KS. The effect of Schistosoma mansoni infection on the response of mice to Salmonella Enteritidis and Listeria monocytogenes. J Infect Dis Infect Dis. 1972;125(3):249–56.
- 19. LoVerde PT, Amento C, Higashi GI. Parasite-parasite interaction of Salmonella typhimurium and Schistosoma. J Infect Dis. 1980;141(2):177–85. pmid:6988520
- 20. Melhem R, LoVerde P. Mechanism of interaction of Salmonella and Schistosoma Species. Infect Immun. 1984;44(2):274–81. pmid:6143728
- 21. Njunda AL, Oyerinde JPO. Salmonella Typhi infection in Schistosoma infected mice. World Am J Microbiol. 1996;15(1):24–30.
- 22. Barnhill AE, Novozhilova E, Day TA, Carlson SA. Schistosoma-associated Salmonella resist antibiotics via specific fimbrial attachments to the flatworm. Parasites and Vectors [Internet]. 2011;4(1):123. Available from: http://www.parasitesandvectors.com/content/4/1/123
- 23. Rocha H, Oliveira MMG, Oliveira VS, Prata A. Almugas caracteristicas da infecçâo por Salmonella Typhi em camundongos com esquistossomose experimental: Multiplicaçâo da bacteria nos Schistosoma mansoni. Rev Inst Med trop Sao Paulo. 1971;13(6):399–404. pmid:5124649
- 24. Mikhail IA, Higashi GI, Edman DC, Elwan SH. Interaction of Salmonella paratyphi A and Schistosoma mansoni in hamsters. Am J Trop Med Hyg. 1982;31(2):328–34. pmid:6803604
- 25. Tuazon CU, Nash T. Interaction of Schistosoma japonicum with Salmonellae and other Gram-negative bacteria. J Infect Dis Infect Dis. 1985;152(4):722–6.
- 26. Tuazon CU, Nash T. Influence of Salmonella bacteremia on the survival of mice infected with Schistosoma mansoni. J Infect Dis. 1985;151(6):1166–9. pmid:3998513
- 27. Tuazon CU, Nash T. Influence of Salmonella and other Gram-Negative bacteria ont the survival of mice infected with Schistosoma japonicum. J Infect Dis. 1986;154(1):179–82. pmid:3086463
- 28. Muniz-Junqueira MI, Prata A, Tosta CE. Phagocytic and bactericidal function of mouse macrophages to Salmonella Typhimurium in schistosomiasis mansoni. Am J Trop Med Hyg. 1992;46(2):132–6. pmid:1539746
- 29. Hsiao A, Toy T, Seo HJ, Marks F. Interaction between Salmonella and Schistosomiasis: A Review. PLoS Pathog [Internet]. 2016;12(12). Available from: e1005928
- 30.
Department of Control of Neglected Tropical Diseases. Schistosomiasis: Progress report 2001–2011 and strategic plan 2012–2020. World Health Organization. 2010. Available from: file:///C:/Users/MSc/Downloads/9789241503174_eng.pdf
- 31. Feasey NA, Dougan G, Kingsley RA, Heyderman RS, Gordon MA. Invasive non-typhoidal Salmonella disease: An emerging and neglected tropical disease in Africa. Lancet. 2012;379(9835):2489–99. pmid:22587967
- 32. Lunguya O, Lejon V, Phoba M-F, Bertrand S, Vanhoof R, Verhaegen J, et al. Salmonella Typhi in the democratic republic of the congo: fluoroquinolone decreased susceptibility on the rise. PLoS Negl Trop Dis. 2012;6(11).
- 33. Kalonji LM, Post A, Phoba MF, Falay D, Ngbonda D, Muyembe JJ, et al. Invasive Salmonella infections at multiple surveillance sites in the Democratic Republic of the Congo, 2011–2014. Clin Infect Dis. 2015;61(Suppl4):346–53.
- 34. Linsuke S, Nundu S, Mupoyi S, Mukele R, Mukunda F, Kabongo MM, et al. High Prevalence of Schistosoma mansoni in Six Health Areas of–Kasansa Health Zone, Democratic Republic of the Congo: Short Report. PLoS Negl Trop Dis. 2014;8(12):8–13.
- 35. Madinga J, Linsuke S, Mpabanzi L, Meurs L, Kanobana K, Speybroeck N, et al. Schistosomiasis in the Democratic Republic of Congo: A literature review. Parasites and Vectors. 2015;8(1):1–10.
- 36. Green SDR, Cheesbrough JS. Salmonella bacteraemia among young children at a rural hospital in western Zaire. Ann Trop Paediatr Int Child Heal. 1993;13(1):45–53.
- 37. Phoba MF, Lunguya O, Mayimon DV, di Mputu PL, Bertrand S, Vanhoof R, et al. Multidrug-resistant Salmonella enterica, democratic republic of the Congo. Emerg Infect Dis. 2012;18(10):1693–4.
- 38.
CDC. Democratic Republic of Congo Country Profile [Internet]. 2018. Available from: https://www.cdc.gov/globalhivtb/where-we-work/drc/drc.html
- 39.
World Health Organization (WHO). Helminth control in school-age children. 2002. Available from: https://www.who.int/neglected_diseases/resources/9789241548267/en/%0D
- 40.
Clinical and Laboratory Standard Institute. Performance Standards for Antimicrobial Susceptibility Testing. 27th ed. In: CLSI supplement M100 Wayne, PA: Clinical and Laboratory Standards Institute; 2017.
- 41.
World Health Organization (WHO). Background document: The diagnosis, treatment and prevention of typhoid fever. 2003. Available from: archives.who.int/hq/2003/WHO_V%26B_03.07.pdf%0D
- 42. Lindstedt BA, Heir E, Gjernes E, Kapperud G. DNA fingerprinting of Salmonella enterica subsp. enterica serovar Typhimurium with emphasis on phage type DT104 based on variable number of tandem repeat loci. J Clin Microbiol. 2003;41(4):1469–79. pmid:12682132
- 43. Hopkins KL, Petres TM, De Pinna E, Wain J. Standardisation of multilocus variable-number tandemrepeat analysis (MLVA) for subtyping of Salmonella enterica serovar Enteritidis. Eur J Infect Dis Epidemiol Prev Control. 2011;16(32).
- 44. Bertrand S, De Lamine de Bex G, Wildemauwe C, Lunguya O, Phoba MF, Ley B, et al. Multi Locus Variable-Number Tandem Repeat (MLVA) Typing Tools Improved the Surveillance of Salmonella Enteritidis: A 6 Years Retrospective Study. PLoS One. 2015;10(2):e0117950. pmid:25693200
- 45. Dimovski K, Cao H, Wijburg OLC, Strugnell RA, Mantena RK, Whipp M, et al. Analysis of Salmonella enterica serovar Typhimurium variable-number tandem-repeat data for public health investigation based on measured mutation rates and whole-genome sequence comparisons. J Bacteriol. 2014;196(16):3036–44. pmid:24957617
- 46.
World Health Organization (WHO). Weekly epidemiological record. Typhoid vaccines: WHO position paper. 2008;83(6):49–60. Available from: http://www.who.int/wer%0A
- 47.
World Health Organization (WHO). Guidelines for the Management of Typhoid Fever. 2011. Available from: apps.who.int/medicinedocs/en/m/abstract/Js20994en/%0D
- 48. Sirinavin S, Pokawattana L BA. Duration of Nontyphoidal Salmonella Carriage in Asymptomatic Adults. Clin Infect Dis. 2004;38(11):1644–5. pmid:15156460
- 49. Buchwald DS, Blaser M. A review of human salmonellosis: II. Duration of excretion following infection with nontyphi Salmonella. Rev Infect Dis. 1984;6(3):345–56. pmid:6377442
- 50. Hathout S el-D, Abd el-Ghaffar Y, Awny A. Salmonellosis complicating schistosomiasis in Egypt. A new clinical appreciation. Am J Trop Med Hyg. 1967;16(4):462–72. pmid:5006466
- 51. Lar PM, Emojevwe ME, Onah JA. Incidence of mixed infections of Schistosoma and Salmonella the Federal capital territory, Abudja. 2006;2(1991):19–24.
- 52. Mohager MO, Mohager SO, Kaddam LA. The association between shistosomiasis and enteric fever in a single Schistosoma endemic area in Sudan. Int J Pharm Sci Res. 2014;5(6):2181–4.
- 53. Salem AK, Bilal NE, Ibrahim ME. Frequent carriage of invasive Salmonellae amongst patients infected with schistosomiasis in Sudan. African J Microbiol Res. 2015;9(8):543–8.
- 54. Im J, Nichols C, Bjerregaard-Andersen M, Sow AG, Løfberg S, Tall A, et al. Prevalence of Salmonella Excretion in Stool: A Community Survey in 2 Sites, Guinea-Bissau and Senegal. Clin Infect Dis. 2016;62.
- 55. Weerakoon K, Gobert G, P C, McManus D. Advances in the Diagnosis of Human Schistosomiasis. Clin Microbiol Rev. 2015;28(4):939–67.
- 56. Coelho PMZ, Siqueira LMV, Grenfell RFQ, Almeida NBF, Katz N, Almeida Á, et al. Improvement of POC-CCA Interpretation by Using Lyophilization of Urine from Patients with Schistosoma mansoni Low Worm Burden: Towards an Elimination of Doubts about the Concept of Trace. PLoS Negl Trop Dis. 2016;10(6):1–13.
- 57. Corstjens PLAM Nyakundi RK, De Dood CJ Kariuki TM, Ochola EA Karanja DMS, et al. Improved sensitivity of the urine CAA lateral-flow assay for diagnosing active Schistosoma infections by using larger sample volumes. Parasites and Vectors [Internet]. 2015;8(1):1–9. Available from: ???
- 58. World Health Organization (WHO). Global Foodborne Infections Network: "A WHO network building capacity to detect, control and prevent foodborne and other enteric infections from farm to table”. 2010;2:43.