Abstract
Rabies is one of the oldest known zoonotic diseases, with dogs being the main reservoir for 99% of the cases of human rabies. However, wild animals may also be rabies vectors. In most cases, contact with a rabid animal results in rabies without pre- or post-exposure prophylaxis, and the disease is nearly always fatal. Nevertheless, a few studies have documented cases of rabies-specific antibodies detection in people with no history of vaccination, suggesting that individuals can be in contact with the virus without developing fatal rabies. To further investigate this possibility of non-lethal human rabies exposure, we carried out a retrospective serological analysis, using both immunoassays (ELISA) and seroneutralization assays (RFFIT), on 430 sera collected between 2005 and 2008 from rural unvaccinated Gabonese populations in the Estuaire and Ogooué-Ivindo provinces. Eleven (11) samples (2.5%) were positive for rabies-specific antibodies using both techniques: 1 in Estuaire and 10 in Ogooué-Ivindo. One of three positive people from the Ogooué-Ivindo province, resampled in early 2023, was still positive for rabies-specific antibodies, suggesting that some degree of immunity can be maintained over many years. Our results also show a marginally significant higher prevalence among hunters. This study demonstrates that rabies circulates actively in Gabon and some unvaccinated individuals living in rural environments can be exposed to the virus and survive, with the development of a significant and specific humoral response that can persist for more than 15 years. This passive seroprevalence survey underlines the need to establish a national surveillance system of rabies in both humans and animals in urban and rural areas, and to enhance access to pre- and post-exposure prophylaxis.
Author summary
Rabies is one of the oldest neglected tropical diseases transmitted to humans, generally by dogs, but wild animals can also act as vectors of the disease. In most cases, a risk-contact with an infected animal without proper prophylaxis results in rabies, and the disease is nearly always fatal. Nevertheless, a few studies have documented the detection of rabies-specific antibodies in people having no history of vaccination, suggesting that exposition to the virus is possible without developing fatal rabies. To further investigate this possibility, we carried out a retrospective serological analysis on 430 sera collected between 2005 and 2008 from rural Gabonese populations. We detected 11 positive samples (2.5%). Three of these positive people was resampled in early 2023 and one was still found positive for rabies-specific antibodies, suggesting that immunity can persist over many years. This study demonstrates that rabies is actively circulating in Gabon and that some unvaccinated individuals living in rural environments can be exposed to the virus and survive. Survival despite exposure to rabies could be associated to the development of a significant and specific humoral response that persists for more than 15 years.
Figures
Citation: Kombila LB, N’dilimabaka N, Lannoy J, Elguero E, Leroy EM, Dacheux L, et al. (2024) Serological evidence of natural exposure to rabies in rural populations in Gabon. PLoS Negl Trop Dis 18(11): e0012044. https://doi.org/10.1371/journal.pntd.0012044
Editor: Prashant Kumar, The University of Kansas, UNITED STATES OF AMERICA
Received: March 5, 2024; Accepted: October 23, 2024; Published: November 14, 2024
Copyright: © 2024 Kombila et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: All data are fully available and can be found within the manuscript and the supporting information files.
Funding: The study was financially supported by the World Organization for Animal Health (WOAH) through the European Union (EBO-SURSY: FOOD/2016/379-660: Capacity building and surveillance for Ebola virus disease), with funds awarded to EML. Additional partial support was provided by the DARRI (Institut Pasteur, Paris), the Institut Carnot "Pasteur Microbe & Santé" (grant INNOV-36-19), and a Programmes Transversaux de Recherche (PTR) grant (PTR 237-19) from the Institut Pasteur, Paris, awarded to LD. The funders had no involvement in the study’s design, data collection and analysis, decision to publish, or manuscript preparation.
Competing interests: The authors have declared that no competing interests exist.
Introduction
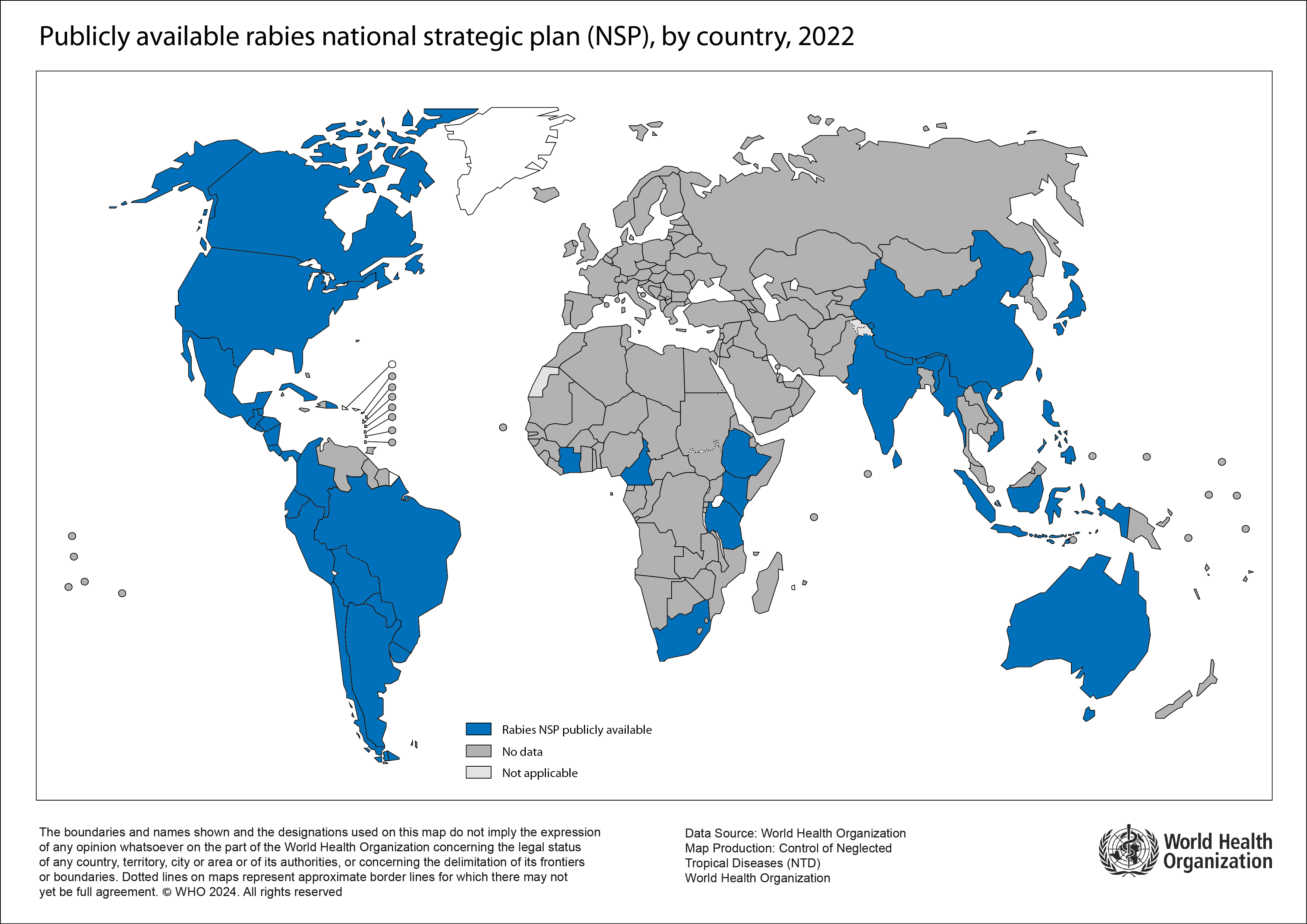
Rabies is one of the most ancient infectious diseases known, with the first suggested descriptions dating from the 4th century BC [1]. This disease is also one of the first to benefit from the development of a specific vaccine, developed by Louis Pasteur and Emile Roux [2]. Unfortunately, rabies still represents a major public health problem, particularly in endemic areas located mainly in low- and middle-income countries. An estimated 60,000 people die each year from this disease, mainly in Asia and in Africa [3], although this figure is probably underestimated and needs to be updated. Indeed, the number of countries presenting publicly available national strategic plans for rabies surveillance and control is still very limited, particularly in Africa.
The etiological agents of rabies are viruses belonging to the genus Lyssavirus within the family Rhabdoviridae. To date, a least 18 different lyssavirus species have been officially recognized, but this number is continuously increasing, with new isolates awaiting classification [4]. Nearly all have been discovered in bats, suggesting that the order Chiroptera represents the original reservoir of these viruses [5]. However, the species Rabies lyssavirus, represented by rabies virus (RABV), is widely distributed in other mammals, especially carnivores, and the domestic dog plays a crucial role in the epidemiology of human rabies [3]. Dogs are the main reservoir and vector of human rabies, transmitting the infection mainly by bites, or in some case through scratches or licking open wounds (as the virus does not pass through the skin intact) and mucous membranes.
Once in the body, the virus can remain at the point of inoculation for some time (incubation period), potentially multiplying in muscle cells or other local tissues. Then, the virus infects motor neuron axons and migrates in a centripetal fashion along the peripheral nervous system, ultimately reaching the central nervous system. Alternatively, it can enter the peripheral or central nervous system directly through decaying or deep wounds [6]. The prodrome stage occurs when the virus replicates in dorsal root ganglia before the syndromic stage, associated with the multiplication in the brain. Two main clinical forms are observed: paralytic and encephalitic forms [7]. Finally, the virus migrates centrifugally from the central nervous system, via the motor and sensory nerves, to innervated and non-nervous tissues. At this stage, the virus is exposed to the immune system and rabies-specific antibodies are detectable in the peripheral vascular system (around 10 days post-infection) [8,9].
In humans, like other mammals (excluding bats), once the first clinical signs appear, the outcome is considered nearly always fatal. Very rare cases of survival after confirmed rabies infection have been described, but most of the time, patients suffer significant neurological after-effects and have a short survival expectancy [10]. To date, there is no treatment for rabies once the symptoms have developed, and post-exposure prophylaxis must be implemented as soon as possible after exposure to rabies. Post-exposure prophylaxis consists in administering a series of rabies vaccines (inactivated virus), with or without serotherapy (human or equine rabies IgG, monoclonal antibodies), depending on the degree of exposure and on previous rabies vaccination (pre-exposure administration or previous post-exposure prophylaxis) [11].
Despite the dogma that rabies is nearly always fatal, the question of whether it is possible to be exposed or even be infected without developing the disease, remains open to debate. Not all cases of exposure to infected animals lead to the development of rabies, because the onset of the disease depends on various factors such as the severity and location of the bite, the viral load and the virus isolates/species. For example, it has been estimated that rabies mortality after untreated bites from rabid dogs varies from 38% to 57% [7]. Similarly, a limited number of studies have investigated the presence of rabies-specific antibodies in the sera of non-vaccinated and healthy individuals [12–23]. In some of these individuals, seropositivity against rabies has been detected, suggesting that they were naturally exposed to rabies, through professional or personal activities, without developing the disease [14–16,19,21,22]. Similar results have also been reported in various mammalian reservoirs and vectors, including domestic dogs and other wild carnivores [24]. However, depending on the study methodology, serological techniques and selected positivity thresholds, results can be difficult to interpret [24].
To extend these studies and further evaluate the possibility of non-lethal exposure to rabies in humans, we carried out a retrospective serological analysi on populations living in two provinces (Estuaire and Ogooué-Ivindo) in Gabon. Despite limited data on rabies circulation in this country due to the lack of rabies surveillance, rabies is considered endemic in the dog population, as in most other African countries [3,6,25]. Although largely underestimated, a few cases of human rabies have also been already described, demonstrating that this disease is present. In humans, previous cases reported to the WHO were diagnosed based on clinical symptoms alone. In 2004, a 3-year-old child with a history of travel to Gabon was diagnosed with furious rabies in France in 2003 [26]. More recently, two cases of human rabies in 2019 and 2020 in the capital Libreville were described and the first molecular diagnosis confirmed the presence of the virus in Gabon [27]. Because both patients had a history of dog bites a few weeks before the onset of symptoms, these animals were likely to be the source of human infection. In enzootic zones, it is also now established that populations are more exposed to rabies in rural areas [6]. However, it is precisely in these areas that access to rabies prevention and vaccination is extremely limited, if not non-existent [25]. In this epidemiological context and using combined serological techniques (ELISA and seroneutralization), we set out to evaluate the presence of rabies-specific antibodies in rural populations, and to demonstrate that some non-vaccinated individuals are seropositive for rabies. Our results show that, likely due to their hunting activities, rural populations may be exposed to rabies without developing an infection.
Materials and methods
Ethics statement
For retrospective samples (obtained during the period 2005–2008), the plasmas were collected as part of an initial clinical study focusing on the Ebola virus, and the related protocol was reviewed and approved by the Gabonese Ministry of Health (authorization nu00093/MSP/SG/SGAQM). Written consent was obtained from the Health Director of each region, the traditional chiefs of each village and each participant. At the time, study was described orally, and volunteers gave their signed informed consent to be enrolled in the study and for their blood samples to be used for future research studies (in link with virus infection).
For prospective samples (obtained in 2023), patients whose rabies serology was positive (by both ELISA and RFFIT tests) and who could be traced using the information available were contacted again, with the agreement of the traditional chief of the village concerned. After reminding them of the context of the initial study that collected their first blood sample (between 2005 and 2008), and of the current study on anti-rabies seroprevalence, they were asked to take a new blood sample in order to assess the persistence of these anti-rabies antibodies. On this occasion, the results of this serology were communicated to them, with a simple information given at the time, specifying that it was an indicator of past exposure to the infectious agent, and not associated with a disease. A new sample was taken only after oral consent had been obtained from the patients concerned.
Study population and samples
To conduct this study, we used retrospective plasma samples from our previous serosurvey conducted from June 2005 to September 2008 throughout Gabon [28]. Two geographical areas were selected for this study. The first area was the province of Estuaire, located in the west of Gabon on the Atlantic coast, which includes Libreville, the capital. This province is characterized by forests, mangroves and savannahs. In 2019 and 2020, two children died of rabies in the Estuaire province [27]. The second was the province of Ogooué-Ivindo, located in the north-east and made up mainly of tropical rainforests. The samples were collected from 100 individuals in 18 villages in Estuaire province and from 332 individuals in 31 villages in Ogooué-Ivindo province (Fig 1). None of the people included in the study had been vaccinated against rabies at the time of sampling. This survey initially focused on rural villages with fewer than 300 inhabitants, which is relevant for increasing the probability of identifying individuals naturally exposed to rabies. During this previous study, all permanent residents aged over 15 years were invited to participate and provide blood samples. Data such as sex, age, province, occupation, hunting activity and village environment were collected to study the risk factors associated with rabies exposure.
The map was created using ArcMap 10.4.1 software. The source of the shapefile for the map background is https://gadm.org/data.html. The source of the routes and waterways is https://extract.bbbike.org/.
Detection of specific anti-rabies IgG using ELISA and seroneutralization (RFFIT)
The detection of specific IgG against the glycoprotein of the rabies virus in plasma samples was conducted using a qualitative enzyme-linked immunosorbent assay (ELISA). The samples were decomplemented by heating for 30 minutes at 56°C, and ELISA was performed using the Platelia Rabies II Kit (BioRad, ref 3551180) according to the manufacturer’s recommendations, with the qualitative method [29]. All samples presenting a signal equal or above the positive control (0.5 equivalent units (EU)/mL) were considered positive. A confirmatory technique was performed using the rapid fluorescent focus inhibition test (RFFIT), as previously described [29–30]. This technique is a cell-based virus neutralization assay used to measure the level of protection against RABV in humans and animals. For this technique, performed in 96-well microplate format, a constant dose of previously titrated, cell culture adapted, RABV challenge virus strain (CVS) is incubated with serial dilution of the sera to be titrated. A reference serum of known titer is included in each test. After one hour of incubation at 37°C, BSR cells (a clone of BHK-21 cells) are added in each well. After 24 h incubation, the estimation of the percentage of infected cells for each dilution of the sera allows determination of the titer of the unknown sera by comparing with the reference serum. The detection and quantification limits of this technique, accredited and implemented according to the ISO 15189 standard, were 0.01 and 0.19 international units per mL (IU/mL), respectively. To avoid false positives and increase the stringency of this test for this study, samples with titer > 0.38 IU/mL (twice the limit of quantification) were considered positive. This test was performed on all ELISA-positive samples, as well as on a random subset of ELISA-negative samples from each province (27 and 40 samples from Ogooué-Ivindo and Estuaire, respectively), in order to validate the RFFIT positivity threshold.
Statistical analysis and software
Forty ELISA-negative samples from Estuaire were randomly selected for seroneutralization using R 4.0.4. The associations at the individual level between the presence of antibodies and sex, age, main occupation (hunter, farmer, others) and hunting activity (professional or otherwise) were assessed using logistic regression. All calculations (odds ratio determination and Benjamini-Hochberg procedure) were performed with the R software and the results of the regression were analyzed for false discovery rate. Figures were produced using ArcMap 10.4.1 and Adobe illustrator 2020 (Fig 1) and GraphPad Prism 10.2.1 (Fig 3).
Results
Description of the population
In Ogooué-Ivindo, a total of 332 plasma samples were collected (Figs 1 and 2 and Table 1). The study population according to sex included 180 (54.2%) men and 152 (45.8%) women. The ages ranged from 18 to 84 years old (mean age of 46.5). The most represented type of village environment was “forest” with 315 people (94.9%). Farmer was the most common occupation, with 204 individuals (61.5%) (Table 1). In Estuaire, a total of 100 plasma samples were collected, and 98 were analyzed (two samples were excluded due to missing data) (Fig 2). The study population according to sex included 50 (51.0%) men and 48 (49.0%) women. Their ages ranged from 18 to 65 years old (mean age of 46.1). The most represented type of village environment was “forest” with 86 people (87.7%). Farmer was also the most common occupation, with 69 (70.4%) individuals (Table 1).
Rabies seroprevalence
Rabies IgG detection using ELISA.
All the selected samples (n = 430) were tested using ELISA based on the qualitative method of the Platelia Rabies II kit to detect IgG specific to the glycoprotein of the rabies virus. A total of 15 samples (3.5%) were considered positive (titer ≥ 0.5 EU/mL) (Table 2).
Confirmation using the RFFIT seroneutralization assay.
Of the 15 ELISA-positive samples, 14 were screened for confirmation using the seroneutralization assay (RFFIT) (12 from Ogooué-Ivindo and 2 from Estuaire). The remaining ELISA-positive sample (#1469–19) could not be tested due to insufficient quantity of plasma (Table 2). Among them, 11 ELISA-positive samples (78.6%) were confirmed with the RFFIT (cut-off value > 0.38 IU/mL) (Table 2 and Figs 2 and 3). The seroneutralization titer ranged from 0.95 to 3.14 IU/mL (median value 1.05 IU/mL).
Green and blue circles correspond to samples from Ogooué-Ivindo and Estuaire provinces, respectively. The red dashed line represents the positive cut-off titer value (> 0.38). Black bar indicates the mean value. Neutralization titers are indicated in international units per mL (IU/mL).
One was from Estuaire, whereas the ten others were from Ogooué-Ivindo (Fig 2 and Tables 1 and 2). The majority of the positive individuals was men (7/11, 63.3%), and lived in forest environment (10/11, 90.9%). The main activities of the positive individuals were farming (n = 5), hunting (n = 4), sawmilling (n = 1), and one was unemployed. Seven of the 11 positive people practiced hunting. When referring to the number of samples initially tested only by ELISA, only samples that tested positive with ELISA and seroneutralization were considered positive. Therefore, the overall positivity rate was 1.0% (1/98) and 3.0% (10/332) for Estuaire and Ogooué-Ivindo, respectively.
Among the random subset of ELISA-negative samples tested to validate the positivity cut-off (27 and 40 samples from Ogooué-Ivindo and Estuaire, respectively), three ELISA-negative samples (3/69; 4.5%) (#20–139, #964–10 and #1021–05) were found positive with the RFFIT, with titers ranging from 0.67 to 1.05 IU/mL (Table 2).
To estimate the persistence of the immune response against rabies, we were able to go back and retest some individuals who had positive ELISA results. Among the 13 ELISA-positive from Ogooué-Ivindo, 3 individuals (#1068–09, #1469–04 and #1469–19) could be resampled in March 2023, and plasma was collected after obtaining their oral consent. None of these three individuals has been vaccinated between the two-sampling dates. Plasmas were tested by both ELISA and RFFIT, and only one (#1469–04), a farmer, tested positive by ELISA, subsequently confirmed by the seroneutralization assay (0.95 IU/mL). The two other samples were negative using both techniques (S1 Fig).
Risk factor analysis
Given the small number of positive samples from Estuaire, statistical analyses were carried out only on Ogooué-Ivindo samples (Table 1). The statistical treatment of all samples (from both provinces) is indicated in Supplementary Information (S1 Table). In Ogooué-Ivindo, only hunting activity was associated with the presence of antibodies (Table 1). The odds ratio associated with hunting calculated from the logistic regression was 4.9, with a 95% confidence interval [1.2–19.5] and a p-value equal to 0.023. After correction for false discovery rate using the Benjamini-Hochberg procedure, the association was no longer statistically significant (effective p-value = 0.092). Statistical analysis carried out on both provinces gave similar results (odds ratio for hunting: 3.8 [1.1–13.3], p-value = 0.035) (S1 Table).
Discussion
Rabies is an infection considered almost 100% lethal once clinical signs appear. However, little information is available on the possibility of exposure to the viral etiological agent (the main one being rabies virus) without subsequent infection leading to the development of disease. To shed light on this aspect of rabies epidemiology, we assessed the existence of natural exposure to non-lethal rabies in unvaccinated populations living in enzootic areas. To reach this goal, we evaluated seropositivity to rabies in retrospective plasma samples collected from rural populations living in two different provinces of Gabon [28]. The first province, Estuaire, features forests, mangroves and savannas, is located in the northwest of the country and includes Libreville; the second, Ogooué-Ivindo province, is located in the northeast and is mainly made up of tropical rainforests.
Our results demonstrate that some unvaccinated individuals can be naturally exposed to rabies and survive, while developing a humoral response to rabies virus that can reach levels comparable to those considered protective by the WHO (≥ 0.5 IU/mL or EU/mL) [11]. To date, only a limited number of studies have detected the presence of seropositivity against rabies in non-vaccinated individuals, suggesting that these individuals had been naturally exposed to rabies without developing the disease [14–16,19,21,22]. This natural exposure to rabies has also been observed in various mammalian reservoirs and vectors, including domestic dogs [24]. However, the results obtained by these studies are difficult to compare, due to the differences between the techniques used and/or the choice of positivity thresholds selected. [24]. Various techniques were used in those previous studies, such as the mouse inoculation test (MIT) [12,13], the complement fixing antibodies test (CF) [18], the indirect fluorescent antibody test (IFA) [21] or seroneutralization assays with the RFFIT [14–17,19–23]. Even for the latter technique, some results were expressed in terms of dilution factor instead of IU/mL [16] or used a lyssavirus other than rabies virus (CVS strain) [23].
Finally, a very small number of studies have been able to detect neutralizing antibody titers in a few unvaccinated patients, in a way that makes comparison possible. For example, during an outbreak of human rabies in two rural communities in the Amazon jungle in Peru, the median titer of seven positive healthy and unvaccinated people (among 47) was 0.18 IU/mL, ranging from 0.14 to 0.66 IU/mL [17]. In another study, only 1 unvaccinated individual out of 21 exhibited a 2.3 UI/mL titer in a trapper community from Alaska, subsequently confirmed by another lab [19]. Investigation of rabies virus exposure in two communities living in the Peruvian Amazon demonstrated the presence of neutralizing antibodies in six unvaccinated individuals, with median 0.5 IU/mL (range 0.1–2.8 IU/mL) [21]. In another study, three individuals exposed to dog meat in Nigeria (butcher or dog meat consumers) had neutralizing antibody titers ranging from 0.65 to 0.7 IU/mL [20], without any antecedent of vaccination. Lastly, a study in Nunavik identified two unvaccinated individuals in a subset (n = 196) of the Canadian Inuit population with titers of 0.51 and 0.71 IU/mL [22]. In comparison, our study reports one of the highest numbers of cases of unvaccinated people seropositive against rabies (n = 11) with neutralizing antibodies titers reaching up to 3.14 IU/mL.
To minimize the difficulties in interpreting this type of result, and ultimately to limit the risk of false positives, we used a combination of two complementary and successive serological techniques—ELISA and RFFIT—in our study. Both techniques have been validated by the WHO for the determination of rabies antibodies after pre- or post-exposure prophylaxis or in cases of rabies infection in humans. Combining these tests also allowed us to measure different characteristics of the rabies humoral response. ELISA detects the presence of specific anti-rabies IgG, whereas the RFFIT test measures the neutralizing activity of antibodies, whatever the class of immunoglobulin considered. In addition, high positive thresholds for each of these techniques were selected. For instance, only plasma samples ≥ 0.5 EU/mL were considered positive (qualitative method of the Platelia Rabies II Kit) for ELISA, whereas this technique has a limit of detection of 0.05 UE/mL and a limit of quantification of 0.125 EU/mL, with ± 0.06 EU/mL uncertainty [29]. Similarly, RFFIT has a limit of detection of 0.05 IU/mL and a limit of quantification of 0.19 IU/mL, with 22% uncertainty, but we set the positive threshold at twice the detection limit (0.38 IU/mL). Therefore, this high level of stringency probably led to an underestimation of seroprevalence. In particular, given the high qualitative ELISA positivity threshold (≥ 0.5 EU/mL), it is not surprising that we detected seroneutralization-positive samples in our subset of ELISA-negative samples (Table 2). Similarly, discrepancies between the ELISA and RFFIT techniques, even if they are limited, do exist, notably because of the difference in methodological approach: the ELISA technique detects anti-rabies IgG whereas the RFFIT technique detects the neutralizing activity of plasma, whatever the immunoglobulin class [29]. The two complementary serological techniques used in this study are based on the use of the RABV CVS strain, limiting the risk of cross-reactivity with another lyssavirus from either of these techniques. However, it cannot be totally ruled out that one of them may also react with a new lyssavirus very similar to RABV. This is particularly true given the fact it that some patients vaccinated with RABV vaccine strain can develop cross-neutralizing antibodies to other phylogroup 1 lyssaviruses [31]. The techniques used in this study cannot assess this exposure, which may contribute to further underestimation of the seroprevalence of this disease, particularly among people regularly exposed to wildlife, such as hunters. The relatively low population size may represent another weakness of this study, because it is not possible to estimate an accurate seroprevalence rate in the two geographical areas of interest. Despite these limitations, our results highlight that some people may have naturally acquired immunity to the rabies virus in these regions.
The existence of patients who have been naturally exposed to rabies and survived, and who develop an efficient anti-rabies humoral response, remains intriguing. The detection of humoral immunity against rabies in unvaccinated and healthy individuals may be the result of an alternative course of rabies exposure [24]. According to Fekadu [32], four scenarios can lead to rabies antibody detection in healthy individuals: subclinical infection, recovery from clinical infection, carrier state, and extended latent period. From all these potential alternative courses, subclinical infection remains the most likely, both in humans and in animals, because it corresponds to a minimal infection sufficient to initiate the development of a specific immune response and to clear the virus before the onset of recognizable clinical symptoms. A fifth possibility may be repeated immunogenic exposure to small amounts of viral antigens, leading to the development of specific humoral immunity, as in rabies vaccination. In humans, these last two alternatives remain closely linked to hunting and farming activities that lead to this type of rabies exposure.
Both of these latter hypotheses are compatible in our study. Positive individuals may have been exposed to rabies virus via saliva, generally through bites, scratches or direct contact of mucous membranes with domestic or wild animals, through their activities and without infection or followed by a short infection. Our results show a marginally significant higher prevalence among hunters, who are more likely to be exposed to the rabies, particularly to wild animals of genera such as Cephalophus or Philantomba (antelopes), Cercopithecus (monkeys), Potamochoerus (bushpigs), Genetta (genets) and bats. Handling these animals may expose the person who caught or prepared them to the virus. Thus, it is possible that rabies antigen stimulation or aborted infection occur when villagers handle animals that have been contaminated by animal saliva and may contain infectious virus particles, inactivated virus particles or simple viral antigens. In addition, bats, which are reservoirs for the virus, circulate at night near homes, and are also eaten by some rural populations in Gabon [33] who would likewise be exposed to the virus. Similarly, individuals with rabies neutralizing antibodies described in previous studies carried out activities at risk of rabies exposure, such as trapping or hunting [19,22], exposure to dog meat [20] or living in remote areas populated by vampire bats in South America [17,21]. Moreover, in our study, three seropositive individuals were found and recontacted in early 2023, almost 15 years later after the first sampling. Among them, anti-rabies IgG were present in one person based on ELISA and confirmed with the seroneutralization assay. Interestingly, this individual, a farmer, has no memory of ever being bitten by a dog or another animal. Although we cannot rule out the hypothesis of minimal or undetected exposure during this period, this result would show that developed immunity can be maintained over many years.
Our results also demonstrate that rabies is present in the rural forest environment in Gabon and may represent a risk to the population, especially people who can be exposed due to their activities such as hunters. However, little information is available on the circulation of rabies virus in dogs, or other lyssaviruses in wildlife, and needs to be further investigated, in particular through the introduction or extension of post-mortem diagnosis of animal rabies on brain biopsy. This information is critical for understanding the transmission of the disease within these populations. In Gabon, vaccination campaigns have already taken place, organized by the Ministry of Livestock, the Ministry of Health and FAO (Food and Agriculture Organization). However, these campaigns are not recurrent and do not cover the entire territory. There is also very little rabies diagnostic capacity (notably the Centre international de recherches mùdicales de Franceville (CIRMF, Franceville, Gabon)), which has a further negative impact on rabies surveillance in Gabon. In addition, access to pre- or post-exposure prophylaxis is very difficult in remote rural areas due to the lack of health centers.
Conclusion
In this study, we demonstrated that some unvaccinated individuals in the rural population in Gabon can be exposed to rabies and survive, and also develop a significant and specific humoral response. Despite the limitations of this study, such as modest sample size and the likely underestimation of the rabies seroprevalence, our results provide evidence for alternative modes of rabies infection in humans, and in particular the potential existence of subclinical infections that can lead to viral clearance with no apparent clinical signs or associated lethality. These results, combined with the few studies describing cases of human or animal rabies, also suggest that rabies is actively circulating in Gabon [27], and stress the need to enhance the surveillance of this disease both in humans and animals, as well as to raise public awareness and to improve access to post-exposure prophylaxis. This last aspect is particularly relevant and achievable with the recent inclusion of human rabies vaccines in Gavi’s vaccine investment strategy, the Vaccine Alliance for 2021–2025 [34]. All these actions are the key to achieving the goal of eradicating dog-related human rabies by 2030 [35].
Supporting information
S1 Table. Descriptive statistical analyses of the combined study population (from provinces of Estuaire and Ogooué-Ivindo, Gabon) according to serological results.
https://doi.org/10.1371/journal.pntd.0012044.s001
(DOCX)
S1 Fig. Distribution of the seroneutralization titers obtained by RFFIT for prospective plasma samples (collected in 2023) and corresponding retrospective plasma samples (when available, collected during the period 2005–2008).
Each color corresponds to plasma samples from a same individual (n = 3). The red dashed line represents the positive cut-off titer value (> 0.38). Neutralization titers are indicated in international units per mL (IU/mL).
https://doi.org/10.1371/journal.pntd.0012044.s002
(TIFF)
Acknowledgments
We thank D. Nkoghe, P. Yaba, A. Delicat, P. Ngari and C. Mbou-Boutambe from CIRMF, Gabon, for their technical assistance during this work. We also thank Carolyn Engel-Gautier for scientific English language editing. The authors also acknowledge the Clinical Research Coordination Office of Institut Pasteur, Paris, and more especially Cassandre Von Platen and Magdalena Stroksztejn for their support with the SeRaGab project.
References
- 1.
Neville J. Historical Perspective of Rabies in Europe and the Mediterranean Basin. OIE, 2004.
- 2. Bourhy H, Dautry-Varsat A, Hotez PJ, Salomon J. Rabies, Still Neglected after 125 Years of Vaccination. PLoS Neglected Tropical Diseases. 2010;4 (11):e839. pmid:21152052.
- 3. Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, et al. (2015) Estimating the Global Burden of Endemic Canine Rabies. PLoS Negl Trop Dis 9(4): e0003709. pmid:25881058.
- 4.
ICTV Taxonomy Release. https://ictv.global/taxonomy.
- 5. Badrane H, Tordo NL. Host Switching in Lyssavirus. History from the Chiroptera to the Carnivora Orders. Journal of Virology. 2001;75(17):8096–104.
- 6. WHO. WHO expert consultation on rabies, third report. 2018.
- 7. Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. Lancet Neurol. 2002;1(2):101–9. pmid:12849514.
- 8. Dacheux L, Reynes JM, Buchy P, Sivuth O, Diop M, Bernard , Rousset D, et al. A Reliable Diagnosis of Human Rabies Based on Analysis of Skin Biopsy Specimens. Clinical Infectious Diseases. 2008;47(11):1410–7. pmid:18937576.
- 9. Dacheux L, Bourhy H. Diagnostic tests for human rabies. Rev Sci Tech. 2018;37(2):581–93. pmid:30747123.
- 10. Fooks AR, Cliquet F, Finke S, Freuling C, Hemachudha T, Mani RS, et al. Rabies. Nat Rev Dis Primers. 2017;3:17091. Epub 20171130. pmid:29188797.
- 11. WHO. Rabies vaccines: WHO position paper–April 2018. Weekly epidemiological record. 2018;16(93): 201–220.
- 12. Ruegsegger JM, Black J, Sharpless GR. Primary antirabies immunization of man with HEP flury virus vaccine. Am J Public Health Nations Health. 1961;51(5):706–16. pmid:13744541; PubMed Central PMCID: PMC1522436.
- 13. Ruegsegger JM, Sharpless GR. Flury rabies vaccine for human use. Arch Intern Med. 1962;110:754–7. pmid:13983161.
- 14. Black D, Wiktor TJ. Survey of raccoon hunters for rabies antibody titers: pilot study. The Journal of the Florida Medical Association. 1986;(0015–4148 (Print)). pmid:3746238.
- 15. Orr P, Rubin M, Aoki F. Naturally acquired serum rabies neutralizing antibody in a Canadian Inuit population. Artic medical research. 1988;(0782-226X (Print)).
- 16. Ogunkoya AB, Beran GW, Umoh JU, Gomwalk NE, Abdulkadir IA. Serological evidence of infection of dogs and man in Nigeria by lyssaviruses (family Rhabdoviridae). Trans R Soc Trop Med Hyg. 1990;84(6):842–5. pmid:2096520.
- 17. Lopez A, Miranda P, Tejada E, Fishbein DB. Outbreak of human rabies in the Peruvian jungle. Lancet. 1992;339(8790):408–11. pmid:1346669.
- 18. Iroegbu CU, Uhuegbu E. Incidence of rabies virus complement-fixing antibodies in unvaccinated dogs, humans and livestock in Anambra State of Nigeria. Microbiologica. 1992;15(2):213–7. pmid:1602992.
- 19. Follmann EH, Ritter DG, Beller M. Survey of fox trappers in northern Alaska for rabies antibody. Epidemiol Infect. 1994;113(1):137–41. pmid:8062870; PubMed Central PMCID: PMC2271209.
- 20. Garba A, Umoh J, Kazeem H, Dzikwi A, Ahmed M, Ogun A, et al. Rabies Virus Neutralizing Antibodies in Unvaccinated Rabies Occupational Risk Groups in Niger State, Nigeria. International Journal of TROPICAL DISEASE & Health. 2015;6(2):64–72. https://doi.org/10.9734/ijtdh/2015/14461.
- 21. Gilbert AT, Petersen BW, Recuenco S, Niezgoda M, Gomez J, Laguna-Torres VA, Rupprecht C. Evidence of rabies virus exposure among humans in the Peruvian Amazon. Am J Trop Med Hyg. 2012;87(2):206–15. pmid:22855749; PubMed Central PMCID: PMC3414554.
- 22. Ducrocq J, Proulx JF, Levesque B, De Serres G, Wood H, Lemire M. Assessment of naturally acquired neutralizing antibodies against rabies Lyssavirus in a subset of Nunavik’s Inuit population considered most at risk of being exposed to rabid animals. Zoonoses Public Health. 2019;66(5):533–9. Epub 20190127. pmid:30688040.
- 23. Vora NM, Osinubi MOV, Davis L, Abdurrahman M, Adedire EB, Akpan H, et al. Bat and Lyssavirus Exposure among Humans in Area that Celebrates Bat Festival, Nigeria, 2010 and 2013. Emerg Infect Dis. 2020;26(7):1399–408. pmid:32568051; PubMed Central PMCID: PMC7323560.
- 24. Gold S, Donnelly CA, Nouvellet P, Woodroffe R. Rabies virus-neutralising antibodies in healthy, unvaccinated individuals: What do they mean for rabies epidemiology? PLoS Negl Trop Dis. 2020;14 (2):e0007933. Epub 20200213. pmid:32053628; PubMed Central PMCID: PMC7017994.
- 25. Mbilo C, Coetzer A, Bonfoh B, Angot A, Bebay C, Cassama B, et al. Dog rabies control in West and Central Africa: A review. Acta Trop. 2021;224:105459. Epub 20200511. pmid:32404295.
- 26. Floret D, Bourhy H, Peigue-Lafeuille H. Don’t forget rabies! Medecine et Maladies Infectieuses. 2005;35:S112–13.
- 27. N’Dilimabaka N, Koumba Mavoungou D, Soami V, Bohou Kombila L, Mouguiama RM, Mondjo A, et al. Molecular analyses of human rabies virus associated with encephalitis in two children in Gabon. IJID Reg. 2022;2:180–3. Epub 20220113. pmid:35757081; PubMed Central PMCID: PMC9216393.
- 28. Becquart P, Wauquier N, Mahlakoiv T, Nkoghe D, Padilla C, Souris M, et al. High prevalence of both humoral and cellular immunity to Zaire ebolavirus among rural populations in Gabon. PLoS One. 2010;5 (2):e9126. Epub 20100209. pmid:20161740; PubMed Central PMCID: PMC2817732.
- 29. Feyssaguet M, Dacheux L, Audry L, Compoint A, Morize JL, Blanchard I, Bourhy H. Multicenter comparative study of a new ELISA, PLATELIA RABIES II, for the detection and titration of anti-rabies glycoprotein antibodies and comparison with the rapid fluorescent focus inhibition test (RFFIT) on human samples from vaccinated and non-vaccinated people. Vaccine. 2007;25 (12):2244–51. Epub 20061227. pmid:17224214.
- 30. WHO. 2018. The rapid fluorescent focus inhibition test, p 196–218. In Rupprecht C, Fooks AR, Abel-Ridder B (ed), Laboratory techniques in rabies, vol 1. World Health Organization, Geneva, Switzerland.
- 31. Wright E, Temperton NJ, Marston DA, McElhinney LM, Fooks AR, Weiss RA. Investigating antibody neutralization of lyssaviruses using lentiviral pseudotypes: a cross-species comparison. Journal of General Virology. 2008 Sep 1;89(9):2204–13. pmid:18753230
- 32.
Fekadu M. Canine rabies. In: Baer G, editor. 2nd edition Boca Raton: CRC Press; 1991. p. pp. 367–87.
- 33. Leroy EM, Kumulungui B, Pourrut X, Rouquet P, Hassanin A, Yaba P, et al. Fruit bats as reservoirs of Ebola virus. Nature. 2005;438(7068):575–6. pmid:16319873.
- 34. WHO, Publicly available rabies national strategic plan (NSP), by country, 2022. https://www.who.int/images/default-source/maps/rabies_national_plan.png?sfvrsn=6e932d_1.
- 35. Nadal D, Bote K, Abela B. Is there hope to reach the Zero by 30 target for dog-mediated human rabies? Lancet Glob Health. 2023;11 (11):e1682–e3. Epub 20230927. pmid:37776869. (4):e0003709.

{kind=link}